ACL Rehab & Returning to Sports
When performing return to sport testing, there are many different options and ways to test your knee. Many clinics will perform 3 tests when assessing return to sport (the single leg single hop, single leg triple hop, and the single leg crossover hop). However, there is much more evidence to support increased testing to minimize the risk of future injury. At peak, we perform a series of tests in the final month of rehab to ensure our athletes are ready to play. We base this series on research and continuously attempt to improve our testing criteria.
The first test/goal we have in ACL rehabilitation is to restore equal range of motion in both your knees. This is an important step to achieve because, while having an ACL reconstruction does not reduce your risk of developing OA in your knee versus nonoperative cases (Friel et all), restoring the full range of motion of the knee after surgery does reduce the risk of developing arthritis (Shelbourne et all). For this reason, we evaluate and equalize your range of motion at the hip, knee, and ankle to minimize the risk of developing osteoarthritis. We test this and aim to achieve it by week 8 with most patients. If you are struggling with knee range of motion, try using the heel prop and heel slide exercises to improve your range of motion:
Heel prop: 
Heel slide: 
Once range of motion is restored, we begin working on assessing the neuromuscular control with the Y balance test. The Y balance test assesses single leg stability by pushing 3 objects as far away from you as possible. We aim to have all the metrics of the Y balance test within 4 cm of eachother side to side to demonstrate a readiness to participate in plyometric training. We aim to have this score by the start of month 3.
Y balance test positions: 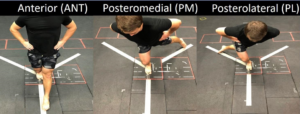
In addition to measuring neuromuscular control, we measure strength at month 3. While most clinics use manual muscle tests – where you resist against your therapist or surgeon’s hand, we prefer a much more objective way of measuring strength. We begin measuring a 5 rep max test with the trap bar deadlift, which is a much better indicator of strength than measuring with your hand. We scale the resistance to the performance of the patient, and make sure our athletes know exactly how to perform the lift before measuring a 5 rep max. This gives us a much better idea of your readiness to progress to the next phase of rehab.
Trap Bar Deadlift: 
Finally, we assess neuromuscular control during plyometrics, or jumping and landing, with the landing error score system. This exam evaluates all your landing mechanics and makes sure you are loading and moving correctly. Certain movement patterns, like demonstrating knee valgus when landing, can predict or increase your risk of re-injury. This exam will be able to identify these movements, and by passing we make sure you understand exactly how to move your body to prevent re-injury and to maximize your performance.
Landing Error Score: 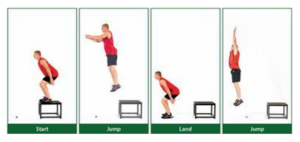
By this point in time, we have concluded the 4th or 5th month of rehab. We have recorded measurements for strength with the trap bar deadlift, neuromuscular control with the y balance test and landing error score system, restored range of motion, and taught the athlete exactly how to move and load their knees safely to minimize risk of re-injury. Once these tests have been completed successfully, we are able to move onto the next phase of PT. This phase will attempt to maximize your strength and equalize your performance with sports specific drills. The final series of tests we use to evaluate the athlete’s movements are as follows:
In order to ensure power production and control, we perform the anterior hop, triple hop, triple crossover hop, timed hop, hop & stop, lateral hop test, vertical jump, and the hop for distance test. While most clinics only perform the first 3-5 tests, we have expanded our testing with single leg stability to ensure we give our athletes the best chance at preventing a re-injury and returning them to sport better than they started.
Hop Tests: 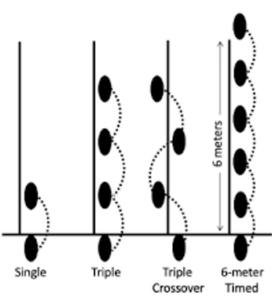
We then assess reactive agility tests. Because all the tests thus far have been tested in a controlled environment, at this point we progress our athletes to be tested in an open environment where they will have to react to the therapist’s movements and complete task oriented tasks similar to sports. During this evaluation which is specific to every athlete’s sport, we are evaluating how effectively the patient is applying the skills we worked on in therapy and demonstrated with the prior testing.
Agility Tests: 
Finally, after all of these tests have been completed, we assess the athlete’s psychological readiness to return to sport. We administer the ACL-Return to Sport After Injury and/or the 2000 IKDC Questionnaire to make sure our athletes are prepared to play. After all these steps have been completed, the athlete is ready to return to sport! While this typically takes 9 months, it can take longer depending on if an athlete needs more time to prepare for their sport.
This battery of tests is supported by research as being comprehensive at assessing an athlete’s readiness for sport. We always strive to give our athletes the confidence to make a full recovery and give them the tools to be confident, and to continue improving after ACL surgery.
Sources:
- Friel NA, Chu CR. The role of ACL injury in the development of posttraumatic knee osteoarthritis. Clin Sports Med. 2013 Jan;32(1):1-12. doi: 10.1016/j.csm.2012.08.017. PMID: 23177457; PMCID: PMC6548436.
- Gustavsson A, Neeter C, Thomeé P, Silbernagel KG, Augustsson J, Thomeé R, Karlsson J. A test battery for evaluating hop performance in patients with an ACL injury and patients who have undergone ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006 Aug;14(8):778-88. doi: 10.1007/s00167-006-0045-6. Epub 2006 Mar 9. PMID: 16525796.
- Nverzagt C, Andreyo E, Tompkins J. ACL Return to Sport Testing: It’s Time to Step up Our Game. IJSPT. 2021;16(4):1169-1177. doi:10.26603/001c.25463
- Shelbourne KD, Freeman H, Gray T. Osteoarthritis after anterior cruciate ligament reconstruction: the importance of regaining and maintaining full range of motion. Sports Health. 2012 Jan;4(1):79-85. doi: 10.1177/1941738111430201. PMID: 23016073; PMCID: PMC3435893.
Comments (0) Trackbacks (0) Permalink