Shoulder Injury Prevention
Shoulder Joint Anatomy and Injury Prevention
No matter how long you have been training or your sport of choice, you may have experienced some shoulder pain or injuries along the way. Let’s find out why.
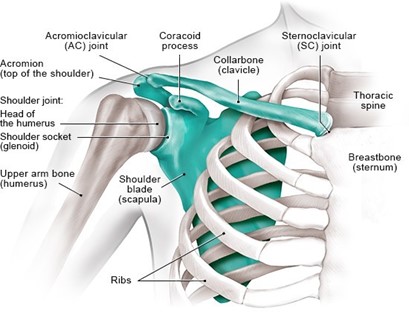
The shoulder joint, or glenohumeral joint, is a complex ball and socket joint, consisting of the head of the humerus (ball) articulating with the glenoid cavity of the scapula or shoulder blade (socket). The shoulder relies on primarily the muscles and ligaments for motion and stability.
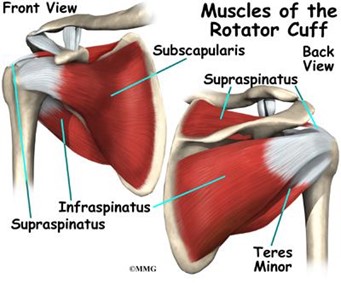 |
The rotator cuff includes four muscles, the subscapularis, teres minor, supraspinatus, and infraspinatus. The acromion or “socket” of the shoulder joint is naturally shallow compared to the size of the humeral head or “ball” of the joint complex. The labrum is a cup-shaped cartilage that acts to deepen the socket and also serves as an attachment site for ligaments and the biceps muscle tendon. |
|
Range of motion of the shoulder is a cumulative effort of a series of multiple joint articulations between the humerus, scapula, clavicle, sternum, thoracic spine, rib cage and rotator cuff muscles.
|
 |
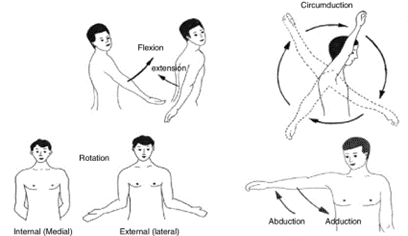 |
Normal Range of Motion
Flexion: 180 degrees Extension: 45-60 degrees Internal Rotation: 70 degrees External Rotation: 90 degrees Abduction: 180 degrees Adduction: 45 degrees |
“What’s Going on with My Shoulder?” Common Diagnoses Explained:
Rotator Cuff Tear: Involves the fraying or full tear of one of the four muscles, with the supraspinatus being the most common site for injury. The tears can be described as a partial or full thickness tear. Typical populations are ages 30-50 years experiencing decreased range of motion, night pain and weakness during active abduction or rotation, or both which can significantly impact daily tasks and recreational activity. Therapy goals would be to improve overall strength with focused exercises on rotator cuff strength as well as mid-back strength and thoracic spine mobility in order to restore full strength through range of motion and prevent future injury.
Atraumatic Instability: Involves normal to excessive motion between the humerus and glenoid cavity that may initially present as the person feeling apprehension with abduction and external rotation or motions that require reaching to the side or overhead. Populations include people ages 10-35 years with no history of trauma. The person may verbalize feelings of slipping, popping or sliding during shoulder motion. Upon assessment, weak muscles around the shoulder blades are typically found.
Subacromial Impingement Syndrome: This occurs when altered joint motion causes impingement or pinching of internal shoulder structures in the shoulder joint. Population includes people 35 years and older. Symptoms can range from mild pain with overhead motion, to moderate pain with range of motion, to pain at rest or at night with observed scapular or rotator cuff weakness.
Frozen shoulder (adhesive capsulitis): This can occur with or without injury to the shoulder. Most common population includes ages 45 years and up. Observation of the shoulder is likely to show a restriction in range of motion of external rotation, abduction and internal rotation. There are three phases: freezing, frozen, then thawing stage. This process can last up to 12-18 months, and physical therapy can assist to decrease this time frame.
“So what should I do to keep my shoulders strong and mobile?”
Here is a series of exercises that promote thoracic spine mobility, scapular muscle strength, rotator cuff strength and improved motion of the shoulder.
| Thoracic Spine Mobility
Begin in a split stance position with your outer leg as the forward leg. Place a towel roll between your front leg and the wall to keep hips centered. Place the inside arm against the wall and use the outside arm as a guide to open up. Use the inside arm as leverage to push further into rotation. Take a deep breath at the end of your rotation to push more into the stretch. Perform 3 sets of 5 repetitions each side. |
 |
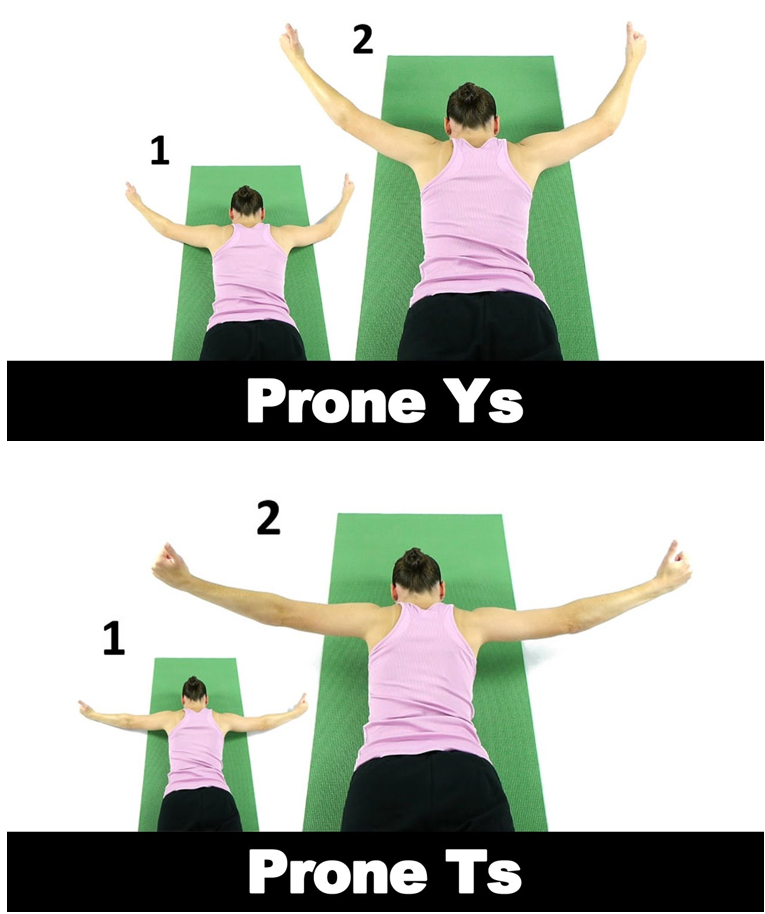
| Ys
Lie on your stomach and lift arms overhead in a “Y” position. Begin with arms resting on the floor then lift up towards the ceiling and hold for 3s then lower slowly back down. Perform 3 sets of 8 repetitions.
Ts Lie on your stomach and lift arms overhead in a “T” position. Begin with arms resting on the floor then lift up towards the ceiling and hold for 3s then lower slowly back down. Perform 3 sets of 8 repetitions. |
 |
| Chest Supported Row
This can be performed with or without weights. Support your chest on the bench and keep your next neutral (look at the floor or rest forehead on bench). Pull hands or weights toward your hips, hold at the top for 3 seconds then lower back to starting position. Perform 3 sets of 8 repetitions. |
 |
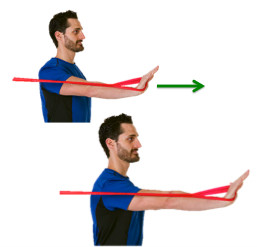
| Serratus Press
Begin by anchoring the band to something sturdy. Hold the band in hand with your elbow in a fixed position. Push against the band by protracting or pushing your shoulder blade forward, then slow retract shoulder down and in. Perform 3 sets of 12 repetitions. |
 |
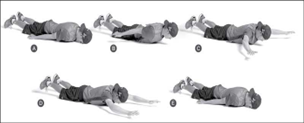
| Snow angels
Begin by lying on your stomach with arms at your side. Lift arms off the floor and continue slow and controlled through snow angel motion until arms are overhead, then slowly return to start position with arms by your side. Perform 3 sets of 8 repetitions. |
 |
References:
- Magee, David J. Othopedic Physical Assessment. 6th Edition. Elsevier Inc. 2014.
Comments (0) Trackbacks (0) Permalink